

Transposition of the Great Arteries Surgical Outcomes

In a healthy heart, the right and left ventricle (the pumping chambers) are each connected to one of the “great arteries” (the arteries that carry blood to the rest of the body) – the pulmonary artery for the right ventricle and the aorta for the left ventricle.
In transposition of the great arteries (TGA), the connection between the pumping chambers and the proper arteries are swapped. There are two main categories of TGA that are treated at Children's National:
- TGA with a ventricular septal defect (TGA with VSD) is a more complex condition where, in addition to the swapped connections, a hole in between the pumping chambers of the heart is also present. TGA with VSD carries a higher risk of mortality, while those with TGA have lower rates of mortality.
- In comparison, TGA with an intact ventricular septum (TGA with IVS) does not have any other issues than the swapped connections and is often called "simple TGA." TGA with VSD carries a higher risk of mortality, while those with TGA with IVS have lower rates of mortality.
The two types are separated in the graphs below because they carry very different risks.
Long-Term Survival Outcomes After Transposition of the Great Arteries Surgery
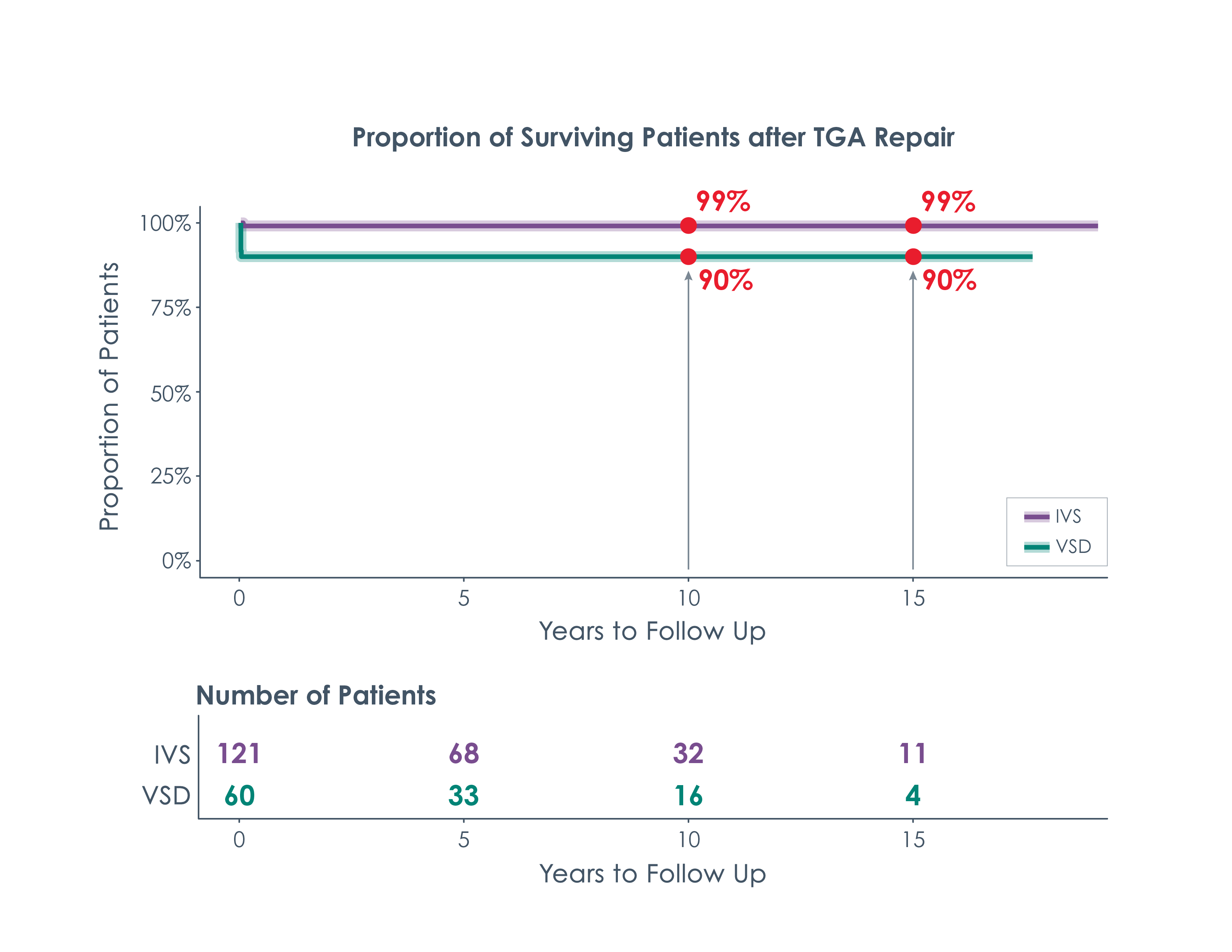
This graph shows the estimated long-term survival rates for people who receive a repair for transposition of the great arteries (TGA) over time. The chart’s two different lines represent the two categories of TGA that are treated at Children’s National – TGA with IVS and TGA with VSD.
The arrows at different time periods show that:
- An estimated 99% of people who had a TGA with IVS repair survive 10 to 15 years after repair.
- An estimated 90% of people who had a TGA with VSD repair survive 10 to 15 years after repair.
Risk of Reoperation for TGA
This graph shows the likelihood that someone who received a repair for transposition of the great arteries (TGA) at Children's National would need to have another surgery (reoperation) within 15 years after their initial surgery.
Reasons for reoperation in people who had TGA correction surgery include:
- The vessel that carries blood from the heart to the lungs becomes too restricted (pulmonary stenosis)— this is the most common reason for reoperation.
- Blood traveling to the rest of the body leaks back into the pumping chamber of the heart (the left ventricle), known as aortic valve regurgitation.
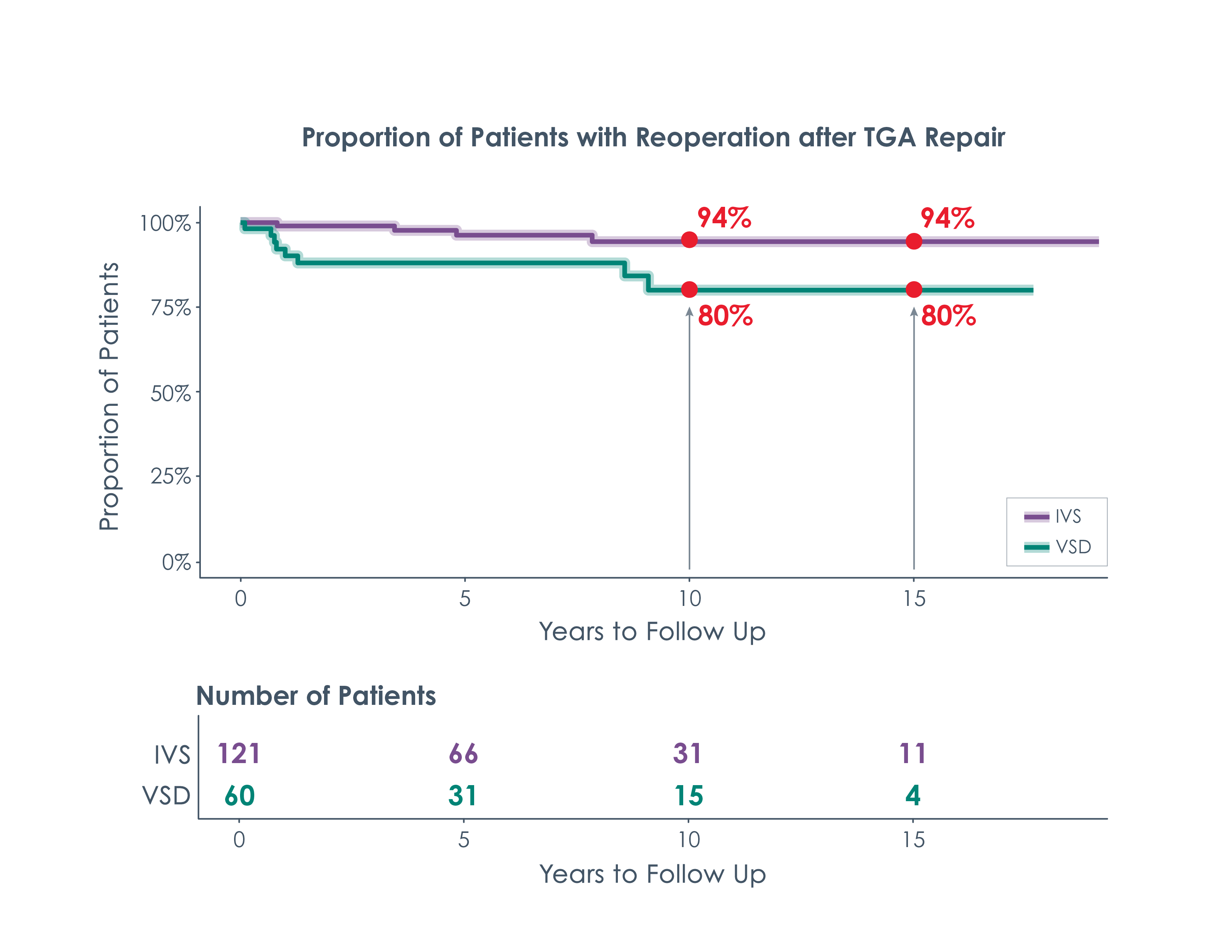
In Figure 2, the graph’s two lines represent the two broad categories of TGA treated at Children’s National – TGA with IVS and TGA with VSD. These are separated because these two types of TGA carry very different risks.
The arrows at different time periods in Figure 2 show that:
- An estimated 94% of people who have had a TGA with IVS repair will not need a reoperation after repair
- An estimated 80% of people who have had a TGA with VSD repair will not need a reoperation after repair
Risk of Cardiac Catheterization for TGA
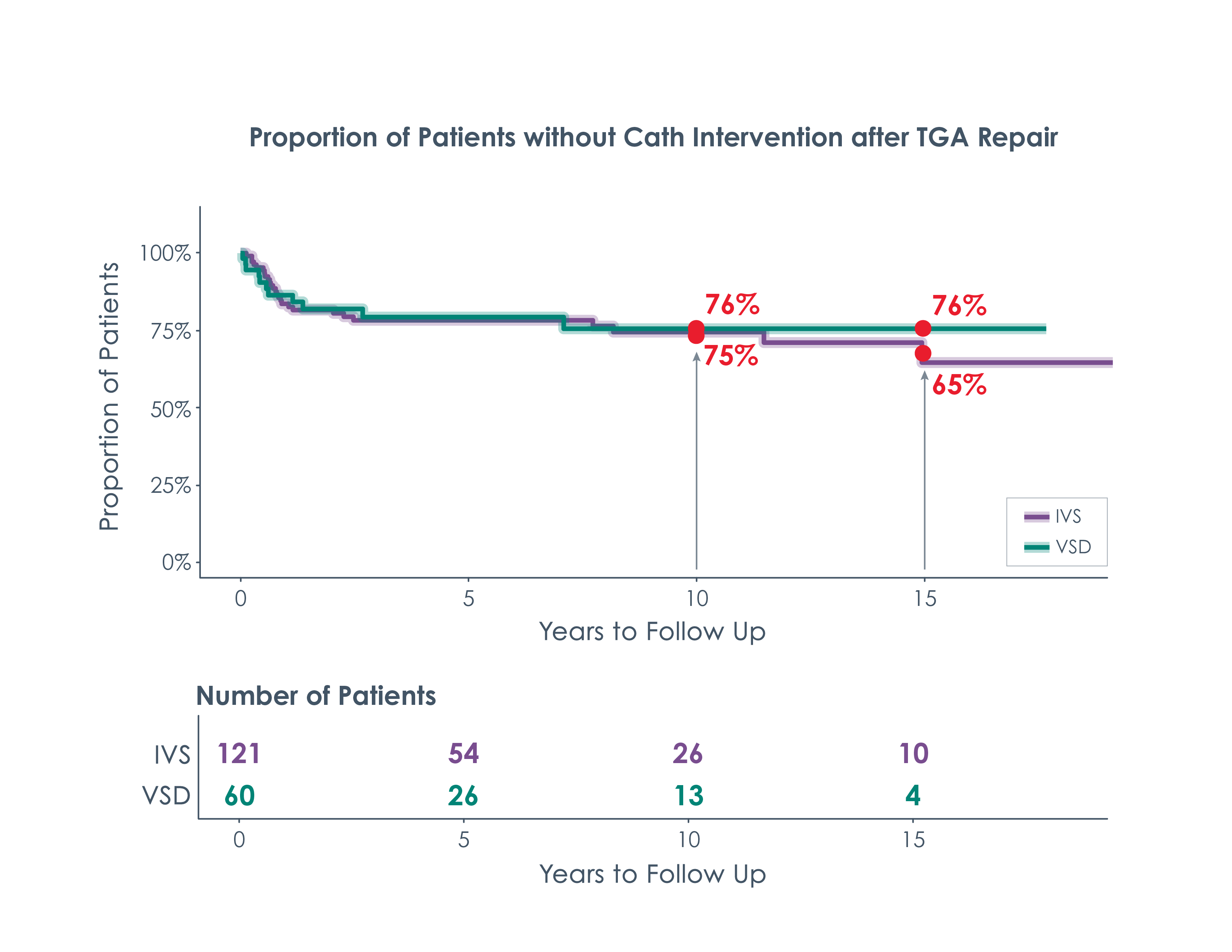
This graph shows the likelihood that someone who received a repair at Children’s National for TGA would need to have a catheter procedure (re-intervention) after a certain amount of time.
The arrows at different time periods show that:
- An estimated 75% of people who have had a TGA with IVS repair will not need a re-intervention 10 years after repair
- An estimated 76% of people who had a TGA with VSD repair will not need a re-intervention after repair
How to Read and Interpret These Numbers
These graphs are called Kaplan Meier curves. They are produced using our own cardiac surgery data that is stored in the CNCORe database. The goal of these graphs is to predict what may happen 10 to 15 years after a child's initial heart surgery. We collect data and information for every single patient we have operated on. Over time, however, some people stop seeing their doctor or move to different states and countries—meaning that researchers do not have complete information for every patient across the years.
The CNCORe data is used to create graphs that estimate risk for something like reoperation using the data we do have, without needing every data point for every single patient.
Understanding the Line Graphs
Cardiac Surgery Long-Term Outcome Graphs
For each heart condition below, you can view data about the risks of surgical procedures and the chances of a child needing additional operations over time.