

Condition
Pediatric Anorectal Malformations
What You Need to Know
Anorectal malformations are birth defects that affect the anus and rectum, causing problems with bowel movements. These malformations are slightly more common in boys than girls.
Symptoms
Symptoms may include:
- Difficulty passing stool or gas
- Abdominal pain
- Constipation
Diagnosis
Anorectal malformations can be diagnosed through a physical exam and imaging tests such as X-rays or ultrasounds.
Treatment
Treatment for anorectal malformations involves surgery to correct the defect and improve bowel function. Follow-up care is important to monitor for potential long-term issues.
What Are Pediatric Anorectal Malformations?
Anorectal malformations occur when a baby’s anal opening, rectum and the associated sphincter muscles and nerves that help the body determine that it is time to go to the bathroom do not develop properly. As a result, the infant is unable to have normal bowel movements, which can lead to a host of other health problems.
Anorectal malformations are congenital defects that occur in developing babies early on in pregnancy. They can range from mild to complex and can develop differently in males and females. Treatment and prognosis will vary depending on the type and severity of the malformation. Early diagnosis and prompt treatment are critical to prevent potential complications.
Pediatric Anorectal Malformation Symptoms
Typically, symptoms of anorectal malformations can be noted shortly after birth. They may include:
- Difficulty or inability to pass stool or gas
- Abdominal pain
- Constipation
- Stomach bloating
- Frequent urinary tract infections (UTIs)
In more severe cases, there may be visible signs such as a missing or malformed anal opening, swelling in the groin area or discharge from the anus. Infants with anorectal malformations may also have other birth defects or genetic conditions that require additional care.
In older children, symptoms may include chronic constipation, soiling (accidentally passing stool or fecal matter) and difficulty controlling bowel movements. Mild cases may not present with any symptoms until later in life.
Diagnosis of Anorectal Malformation in Infants
An anorectal malformation is usually diagnosed through a physical examination and imaging tests. These can include X-rays, ultrasounds or a fluoroscopic study to evaluate the anatomy of the anus and rectum.
In some cases, further testing may be necessary to rule out other potential causes for symptoms or to determine the extent of the defect. This may involve consultations with specialists such as pediatric urologists or geneticists.
Types of Anorectal Malformations
There are several types of anorectal malformation, each of which has its unique characteristics. Doctors typically classify malformations based on where the rectum ends in the abdomen and if there is a fistula – an abnormal connection that develops between organs which can cause stool to pass into other parts of the abdomen. Types of anorectal malformations include:
- Cloacal malformation. The vagina, rectum and urinary tract are combined into a single channel.
- Imperforate anus. The anal opening is missing or blocked.
- Rectal atresia. The rectum does not connect to the anus.
- Rectal stenosis. The anus or rectum is too small to allow stool to pass.
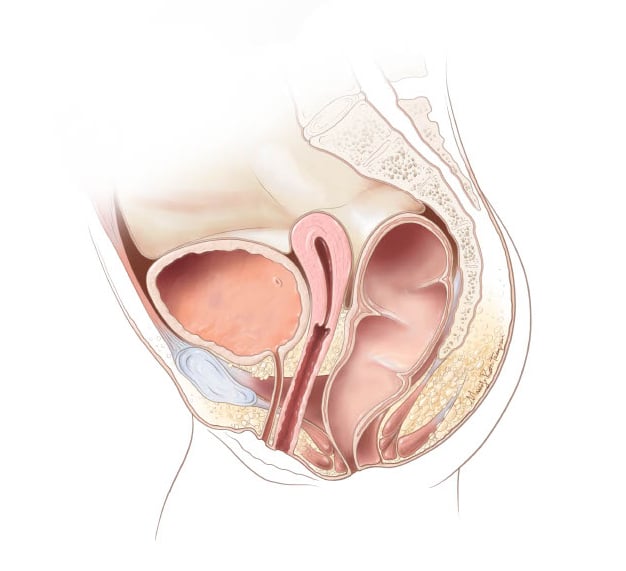
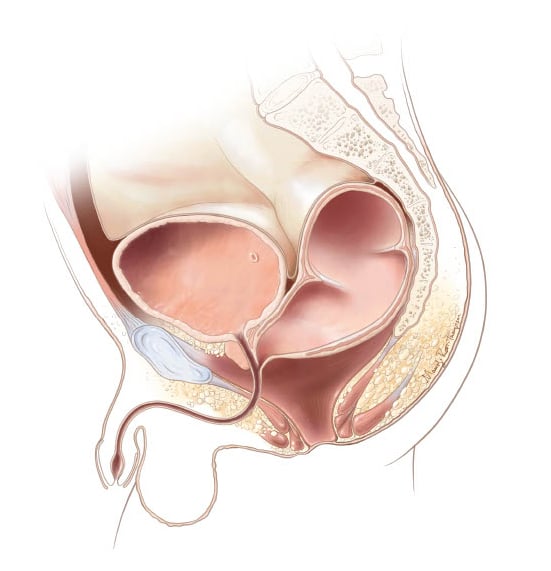
Types of Malformations
Rectovestibular fistula
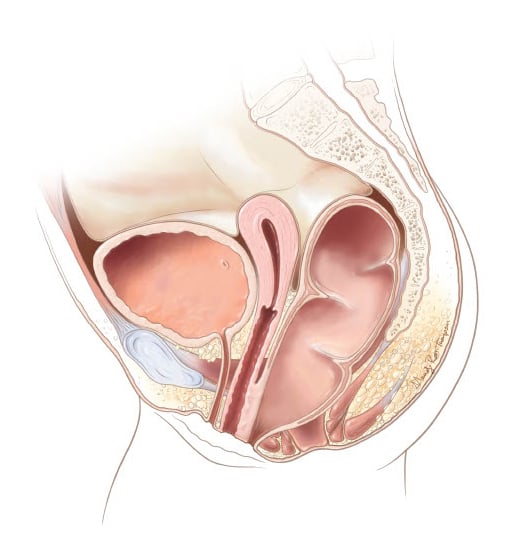
Variations of the distal rectum
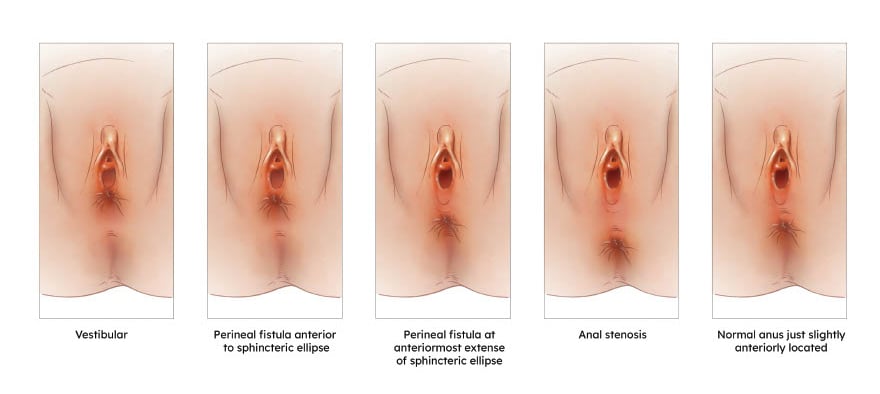
- Vestibular fistula
- Perineal fistula with the fistula exiting anterior to the sphincteric ellipse in the perineal body
- Perineal fistula with the fistula exiting within the sphincteric ellipse, at its most anterior extent
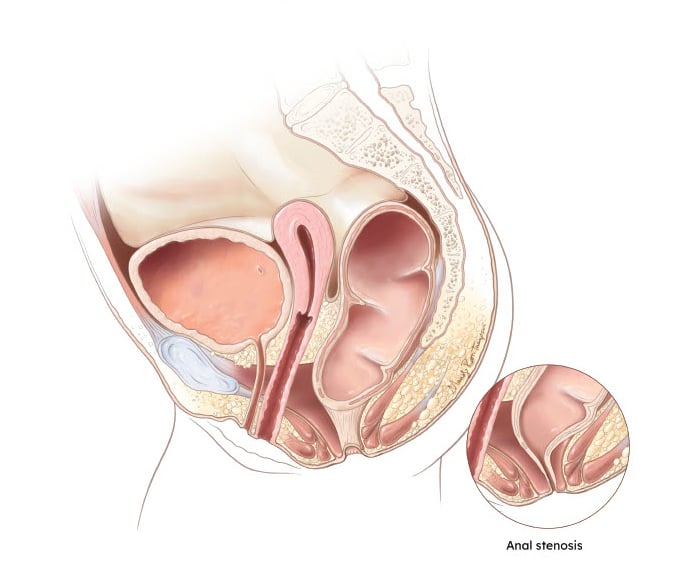
- Anal stenosis – a narrow opening at the center of the sphincteric ellipse
- A normal anus in size and located within the sphincteric ellipse, but anteriorly located with a smaller perineal body
Anal stenosis in a female
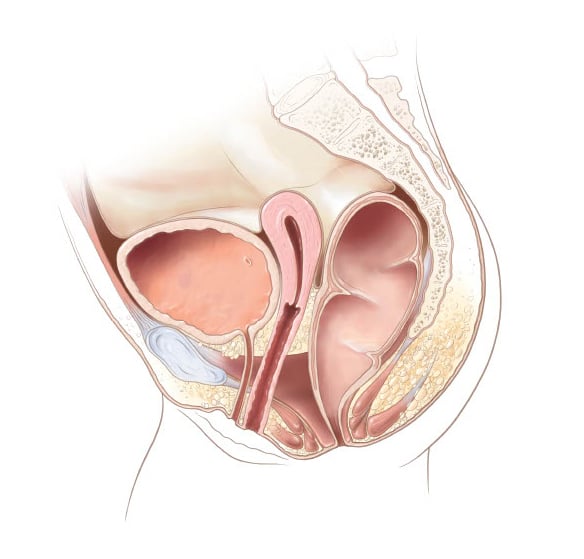
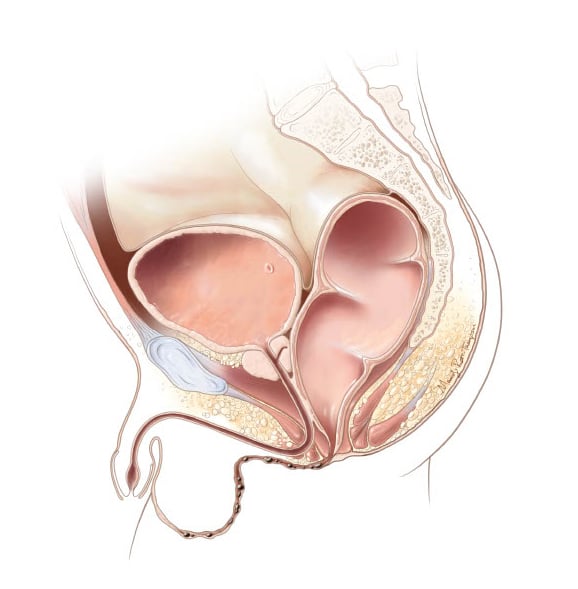
Rectoperineal fistula in a female 1
The distal rectum exits as a fistula into the perineal body.
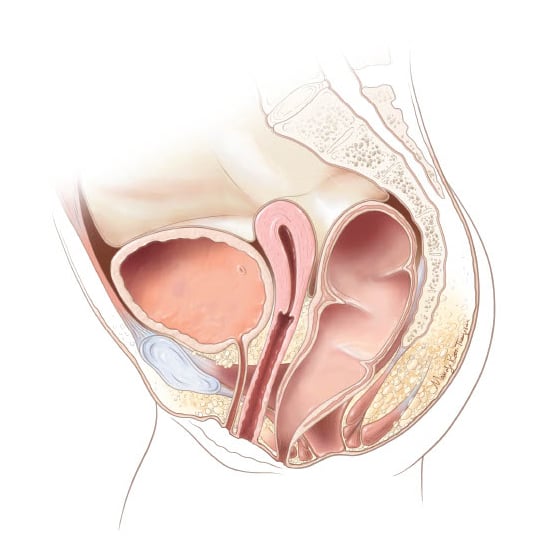
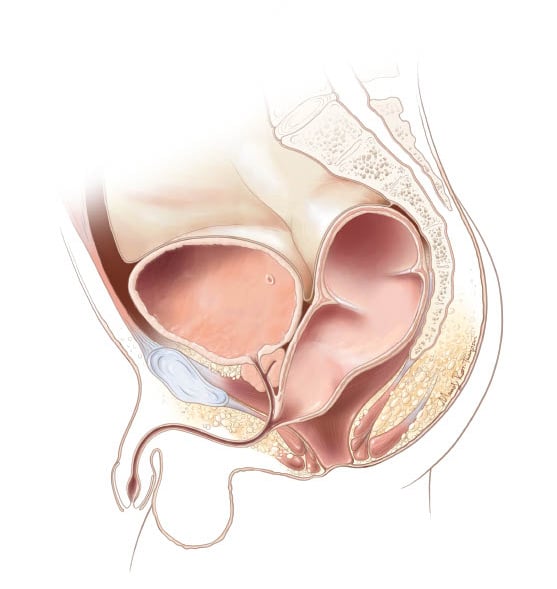
Rectoperineal fistula in a female 2
Rectal altresia-stenosis
.jpg?h=568&iar=0&w=578&rev=65b01b777fb048ce870da390bb889e86)
Treatment of Pediatric Anorectal Malformations at Children's National
Most babies with anorectal malformation will need one or more specialized surgeries to correct the problem. Our highly experienced colorectal surgeons are trained in the latest surgical approaches for all types of anorectal malformations, including implementing leading-edge, minimally invasive techniques. In fact new operations for male and female patients with rectoperineal fistula were developed first at Children’s National.
Treatment for anorectal malformations will depend on the type and severity of the defect. In most cases, surgery is necessary to correct the defect and improve bowel function. Our team at Children’s National has extensive experience performing surgeries for anorectal malformations, the largest in the world, including complex cases that require multiple procedures.
In some cases, a temporary ostomy may be necessary to allow the intestines time to heal before proceeding with reconstructive surgery. This involves creating an opening in the abdominal wall through which feces can exit into a bag outside of the body until a later procedure can be performed.
Surgical Repair for Anorectal Malformation
Colostomy
Posterior Sagittal Anorectoplasty (PSARP)
Colostomy Closure
Caring for Your Child After Reconstructive Surgery for an Anal Malformation
Learn how to care for your child after reconstructive surgery. Before performing any of steps from this video, consult your child's pediatrician.

Post Operative Skin Care After Colorectal Surgery
The goal of this video is to teach you how to care for your child’s skin on their bottom after surgery. We want to prevent and treat any skin breakdown that happens due to the presence of stool on the skin.

How to Perform a Rectal Enema on Your Child
Learn the right way to administer an enema. An enema will clean your child’s colon of stool. We want this to be a good experience for you and your family.

How to Perform an Anal Dilation on Your Child
The goal of this video is to reach you how to perform anal dilations to either prevent or treat narrowing of your child’s anus so that additional surgery may not be needed.

Explore Conditions that Can Develop with Anorectal Malformations (ARM)
On-going follow-up care, careful monitoring and addressing certain urologic and gynecologic issues that develop in children with ARM early on is key to reducing the risk of developing certain problems and conditions later in life.
Recovery from Anorectal Reconstructive Surgery
Recovery from anorectal reconstructive surgery will typically require two to four days in the hospital. For several months after surgery, anal dilations may need to be performed to help stretch the anus to the appropriate size for your child’s anatomy and age. Although surgery restores some function, the nerves and sphincter muscles your child relies on to let them know they need to go to the bathroom may be weak.
You can best help your child regain normal bowel control by following your doctor’s recommendations. To keep your baby comfortable and prevent constipation after surgery:
- Feed them a high-fiber diet (if they are old enough to eat solids)
- Encourage adequate hydration
- Avoid foods that tend to cause firm stools, such as dairy products
As you work with your surgical team on your child’s postoperative care, we’ll provide you with detailed instructions tailored specifically to their condition.
After surgery, some children may still face challenges such as constipation, soiling and difficulties with potty training. Fortunately, these issues can be effectively managed through a bowel management program. This program can help restore your child's optimal function and strengthen their muscles post-surgery. To address constipation, it's essential to maintain a balanced diet rich in fiber, along with laxatives if necessary. It's important to consult with your surgeon to understand what recovery will entail for your child.
Long-Term Outlook for Children with Anorectal Malformations
The long-term outlook for children born with anorectal malformation is generally positive. Most children will experience improved bowel function and control after surgery and can lead a healthy, active life.
As the child grows, they may need additional surgeries or procedures to address any ongoing issues such as constipation or incontinence. Regular follow-up appointments can help monitor their progress and address any concerns that may arise.
It's important to remember that each child's case is unique, and individual outcomes may vary. However, with proper medical care and support, children born with anorectal malformations can thrive and live fulfilling lives. As a parent or caregiver, it's essential to advocate for your child's needs, work closely with their medical team, and provide them with love and support as they navigate this condition. Some patients require a bowel management program as they reach potty training age. With compassion and expert care, we can help children with anorectal malformations reach their full potential.
Schedule a Visit with One of Our Anorectal Malformation Specialists
If your child has been diagnosed with anorectal malformation, our team is standing by to provide specialized care.
Meet the Providers Who Treat Anorectal Malformations
Our providers are specifically trained to care for the needs of children with anorectal malformations, providing expert care when your child needs it most. Get to know our team.


Departments that Treat Anorectal Malformations

Pediatric Colorectal & Pelvic Reconstruction
The Division of Pediatric Colorectal & Pelvic Reconstruction offers the latest advancements in diagnosis and treatment for all types of pediatric colorectal disorders. Learn more about our division.




Help Kids and Make a Difference
Invest in future cures to help children have brighter futures.