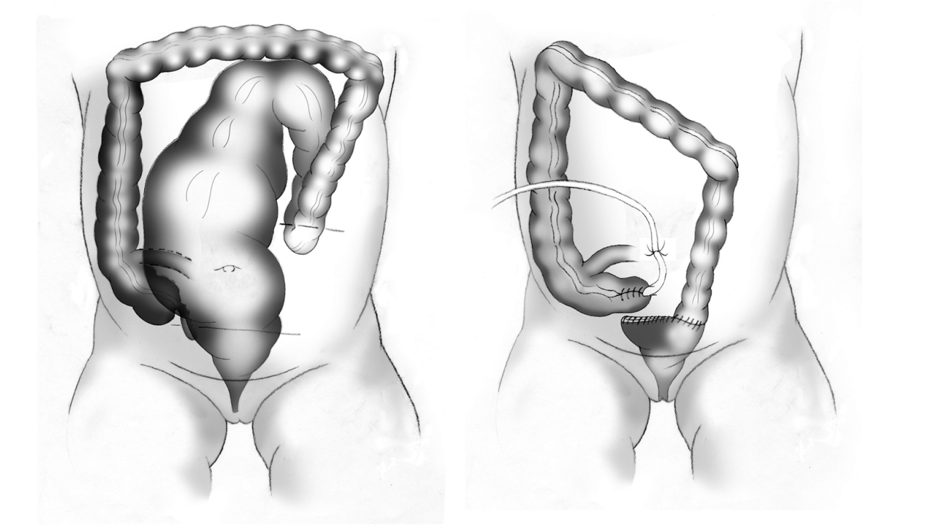
An antegrade continence enema (ACE) procedure, also known as a Malone procedure, is a surgical procedure that involves constructing a tube from the appendix through the belly button through which an enema can be given. This provides an alternative route for the enema, and can more easily be performed by the patient, promoting their independence.
This operation is usually recommended for patients who are capable of being more independent, as it allows the administration of the enema without parental assistance. It should ideally be performed in patients for whom bowel management has been successful. However, for children who cannot tolerate rectal enemas, this procedure is also beneficial as a bridge to continence, enabling the training of the sphincter muscles while the patient tries to hold onto the flush.
Malone Appendicostomy Procedure:
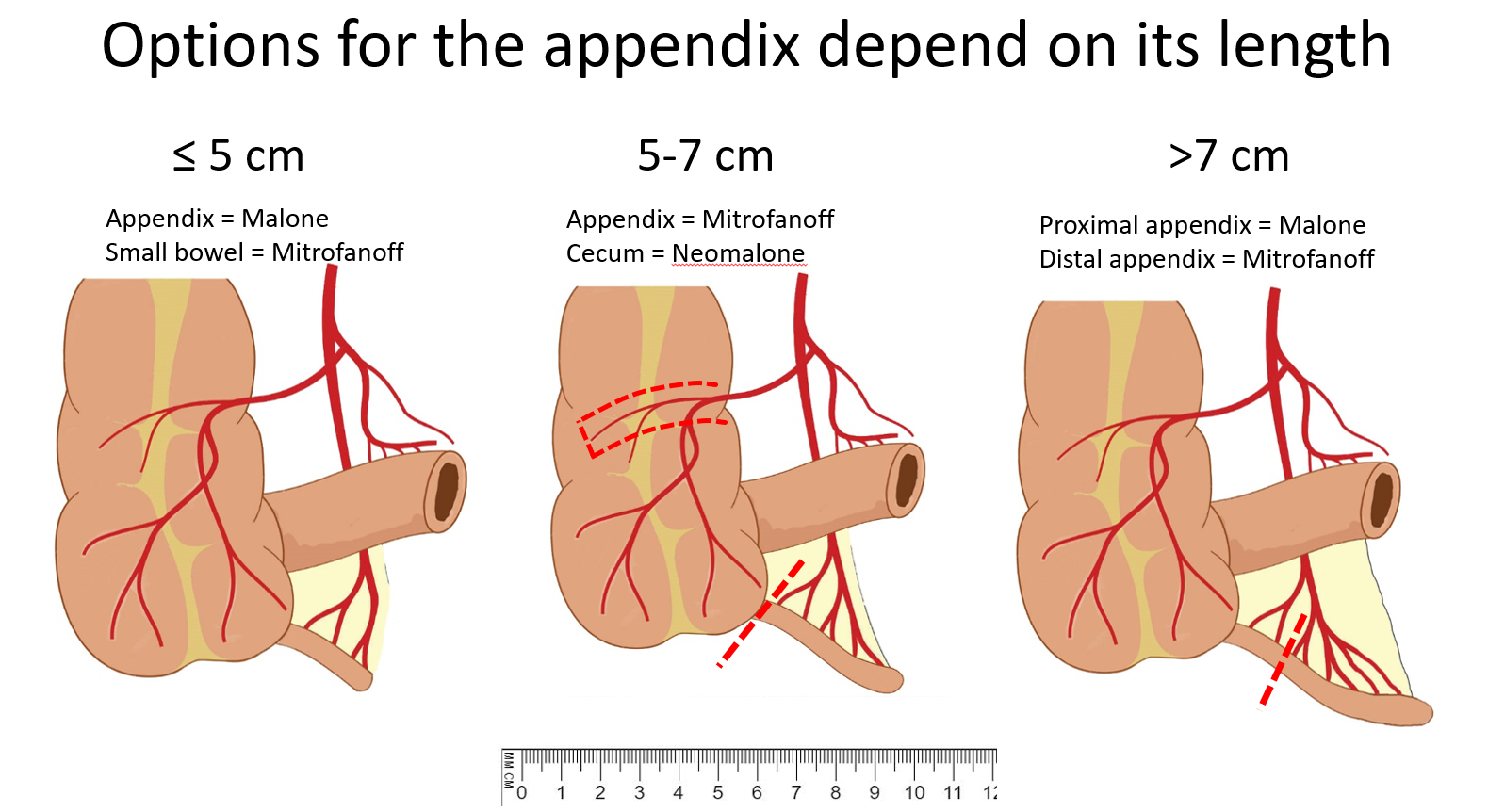
In patients in whom both a Malone appendicostomy and a similar tube construction for the bladder and urinary system are needed, there are various strategies that may be employed to share the appendix, which depends on whether the appendix is a certain length: