Treatment
Pediatric Pacing and ICD Lead Extraction
What is a pacing or ICD lead?
A lead is a thin, flexible wire inserted in an upper extremity vein and directed to the top chamber (atrium) or the bottom chamber (ventricle) of the heart. The lead delivers energy to the heart muscle from a pacemaker or implantable cardioverter defibrillator (ICD) – special devices implanted under the skin that help keep the patient’s heart beat in a regular rhythm.
Frequently Asked Questions
What is lead extraction?
When the leads are initially inserted through the veins of the chest and implanted into the heart, they can be easily removed. However, eventually the leads are held in place by scar tissue (Figure 1).
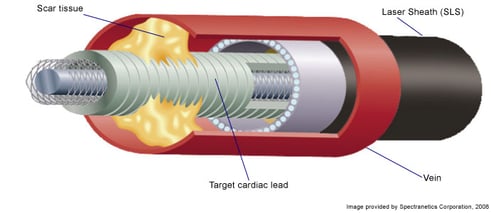
Lead extraction is the removal of one or more leads from the inside of the heart and veins with special tools that safely release the lead from the scar tissue binding the lead in place.
Why is lead extraction necessary for a child?
Despite advances in lead design, pacing leads may become non-functional. Reasons include too high an energy level required to stimulate the heart, too small a signal coming back from the heart so the pacemaker can not “sense” electrical activity from the heart, lead fracture, or infection. A lead must be removed when it becomes infected or causes a mechanical problem in the heart.
Class 1 indications – almost all physicians agree that the procedure will benefit the patient.
- Documented infection of heart and any intravascular portion of the pacing system
- Infection of the pacemaker pocket when the intravascular portion of the lead system cannot be aseptically separated from the pocket
- Obliteration or occlusion of all usable veins, with the need to implant a new transvenous pacing system
- Life-threatening arrhythmias secondary to a retained pacing lead fragment
- A retained lead that poses immediate or imminent physical threat to the patient
- Clinically significant thromboembolic events caused by a retained lead
- A lead that interferes with the operation of another implanted device
Class 2 indications – most physicians agree that the procedure will benefit the patient.
- Non-functional leads in young patients
- Leads preventing access to the venous circulation for newly required implantable devices
- Localized pocket infection, erosion or chronic draining sinus not involving the transvenous portion of the lead system (when the lead can be cut through a clean incision that is totally separated from the infected area)
- A lead, due to its design or its failure, may pose a threat to the patient, though it is not immediate or imminent if left in place
- Chronic pain at the pocket or insertion site not manageable by medical or surgical technique without lead removal
Class 3 indications – general agreement that lead removal is unnecessary.
How can I prepare my child for a lead extraction procedure?
- Ask your child's doctor what medications they are allowed to take. Your doctor may ask your child to stop certain medications one to five days before your test (aspirin, ibuprofen and coumadin).
- Your child should not eat or drink anything after midnight the evening before their test (Eight hours prior to your procedure). If they are asked to take some of their medications, they can drink only with a sip of water.
- When you come to the hospital, make sure your child wears comfortable clothes. They will change into a hospital gown for the procedure. Leave all jewelry or valuables at home.
- Your child will need to stay in the hospital for 48 hours after the procedure.
What to expect when your child comes to the hospital?
- Your child will be given a hospital gown to wear.
- Your child will lie on a bed and the anesthesiologist will start an intravenous (IV) line in your arm so that medications and fluids can be administered during the procedure.
- Your child's technicians will connect them to several heart and blood pressure monitors.
- Your child may feel nervous. They will be given general anesthesia so they are sleeping during the procedure and will not feel any pain or discomfort.
- Your child's chest and both groins will be shaved and cleansed with an antiseptic solution. Sterile drapes are used to cover them from their neck to their feet to prevent infection. It is important that your child keeps their arms and hands down at their sides and not disturb the drapes. To remind them, some type of restraint may be used to prevent their hands from coming in contact with the sterile field.
- While your child is asleep, a catheter will be placed in their bladder to drain their urine.
- The lead extraction can be performed at two sites:
- Subclavian vein. Most frequently used. An incision is made in the upper chest over the subclavian vein.
- Femoral vein. Used when the subclavian approach cannot be performed. A small puncture (instead of an incision) is made in the groin over the femoral vein.
- A sheath (plastic, hollow tube) is placed in the vein, and guided to the tip of the lead (where the lead attaches to the heart). The sheath helps to free the lead from sites at which the lead is bound to the vein or heart wall.
- A special laser sheath is used to deliver energy to remove scar tissue from the lead.
- New leads may be implanted (placed in your heart) during this procedure or at a later date. This will depend on why the old leads were being removed.
- A lead extraction procedure takes about four to six hours to perform.
What happens after my child's lead extraction procedure?
- You will be admitted to the hospital for 48 hours to be given intravenous antibiotics to try to prevent infection. You will be placed on a monitor called telemetry that allows your heart rhythm to be displayed on monitors in the nursing unit – Cardiac Intensive Care Unit (CICU) or the Heart – Kidney Unit (HKU).
- If you had new leads and a pacemaker implanted, you will also have a Holter monitor applied to record your heart rhythm overnight. This is another way to check proper pacemaker function.
- The arm on the side at which the lead extraction procedure was performed will be placed in a “sling” to remind you not to move it above shoulder level.
- If the femoral approach was used, you will need to lay flat (your head can be elevated 30°) in bed for six hours after the procedure.
- The morning after your lead extraction procedure you will have a pacemaker check to assess the function of your new pacing leads and pacemaker.
- Before you leave the hospital, your doctor and nurse will talk to you about activity, medications or any follow-up appointments.
- You will return to the clinic in two weeks for a wound check and in one month for a repeat wound check and a check of your pacing system. You may be asked to come back for additional follow-ups.
- Once you are home, we advise you to follow general health guidelines, including eating a heart-healthy diet. If there are no complications from the procedure, you should be able to return to school or work in three to 10 days.
What are the techniques for lead extraction in children?
Techniques for dealing with failed pacing leads have evolved over time. Initially, non-functioning pacing leads were abandoned and left in the pacemaker pocket and a lead cap was applied to the lead tip if it was not critical to remove the pacing lead. If necessary but not critical to remove the pacing lead, weights were applied to the end of the lead to apply constant outward traction to facilitate lead removal (Figure 2).
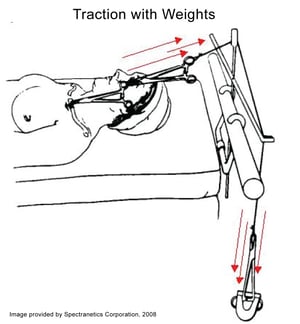
This technique frequently resulted in a part of the heart muscle wall being avulsed (torn away) and removed with the lead. Tearing of the heart muscle wall may lead to fluid collection around the heart (pericardial effusion). When absolutely necessary to remove non-functioning pacing leads, open heart surgery was resorted to.
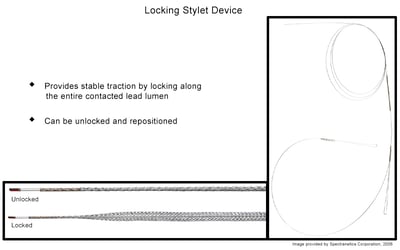
In the 1990’s, tools were developed to facilitate the mechanical extraction of pacing leads. The tools included counter-traction with mechanical sheaths (plastic tubes) to avoid the problem of ripping the heart muscle wall, telescoping mechanical sheaths, and locking stylets (Figures 3 , 4 and 5).


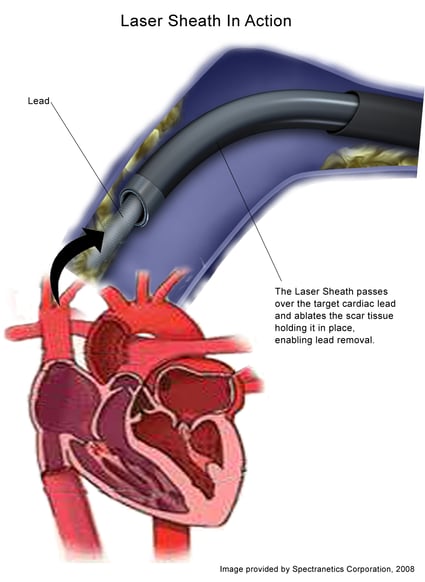
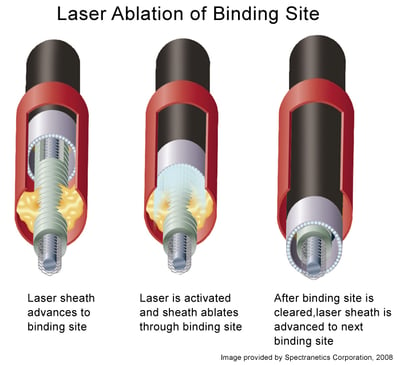
While very effective in removing pacing leads, these tools were difficult to use and made the procedure very time consuming. In the late 1990’s, sheaths were developed that had laser fibers at the tip to allow local delivery of laser energy at the site of scar tissue binding the pacing lead in place (Figure 6).
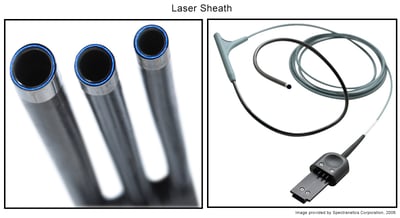
At sites of lead binding a pulse of laser energy is applied that results in freeing of the lead – dissolution of the scar tissue holding the lead in place, facilitating advancement of the sheath. The sheath is gradually advanced to the lead tip (Figure 7).
Using counter-traction techniques, the lead tip is eventually freed and the lead can be removed through the sheath.
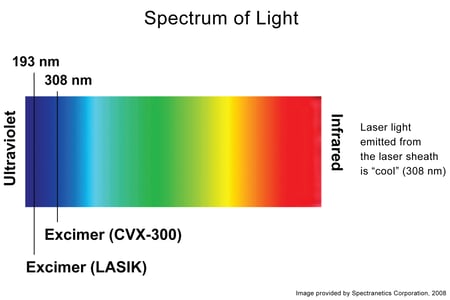
The laser sheath is connected to an Excimer laser system that uses xenon chloride gas, and emits a pulse of light energy at a wavelength of 308 nm (in the ultraviolet spectrum), with a depth of penetration of only 50 microns (Figure 8).
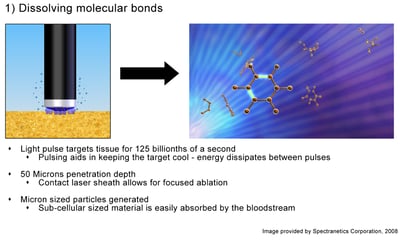
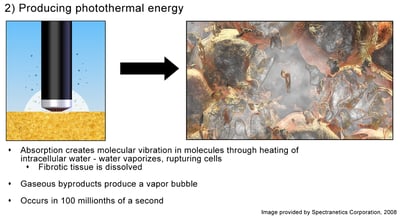
The laser energy “ablates” the scar tissue through 3 mechanisms of action: 1) photochemical – dissolution of chemical bonds, 2) photothermal – heating created through photo heating process of intracellular water, and 3) photomechanical – creating kinetic energy (Figures 9), (10 and 11).
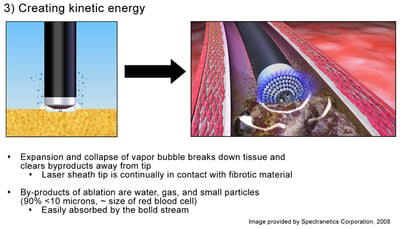
The doctor first makes a 5-centimeter incision on the side of the chest where your child's pacemaker or ICD incision was made. Through this incision, the doctor removes the battery from your child's pacemaker or ICD and disconnects it from the pacing lead. Scar tissue holding the pacemaker and leads in place is dissected to free them up from inside the pacemaker pocket. Then, the doctor places the laser sheath over the lead that needs to be removed and directs the sheath inside the vein. The laser sheath is guided down to the tip of the lead, where it attaches to the heart. The sheath helps stabilize the heart muscle while the lead is removed. The sheath is attached to a laser. The laser delivers energy to remove the scar tissue holding the lead in place – either in the vein or around the tip of the lead (Figure 12).
This detaches the lead from the inside of the vein and at the tip of the lead. The doctor then removes the lead from the sheath, and may implant a new lead right away, or wait to a later date if your child has an infection of the pacing system.
What are the outcomes of lead extraction surgery in children?
Lead extraction is a very effective technique. Complete lead removal is accomplished in 93% of leads. Sometimes a small fragment of the pacing lead tip is left behind (5%). This is usually not a clinical problem and will not interference with the mechanical or electrical activity of the patient’s heart. Small lead fragments can be left in place without any danger to the patient or any known long term complications. Failure of lead extraction occurs in 2% of cases. Extraction of pacing leads can allow venous revascularization and implantation of a new pacing or ICD lead, avoiding the use of alternative venous access sites or cardiac surgery. Venous revascularization may necessitate balloon angioplasty of the vein in which the lead is implanted and the veins leading to the heart and possible stent implantation to keep the vein(s) open.
What are the complications of a lead extraction procedure in children?
Complications are uncommon, in experienced hands, and may include infection, bleeding from the vein or heart (vascular tear or perforation), pneumothorax (air collection around the lung), arteriovenous fistula formation and pulmonary embolism (blood clot to the lung). Predictors of major complications are a longer period of the lead having been implanted (5 or more years), female gender, multiple leads and ICD leads. Major complications occur in 1-3% of procedures. Death has been reported in 0.5-1.0% of procedures. We usually have a cardiovascular surgical team on standby in case any urgent major complication develops.
Providers Who Offer Pacing and ICD Lead Extraction
Departments that Offer Pacing and ICD Lead Extraction

Heart and Lung Center
Our expert pediatric heart team, including more than 40 subspecialties, offer advanced heart care and excellent outcomes for thousands of children every year.

Cardiology
The pediatric heart experts at Children's National Hospital in Washington, D.C., provide advanced cardiology care for unborn babies, children and young adults with heart conditions. Learn more about this program.

Cardiac Catheterization
We perform hundreds of catheterization procedures every year. We treat children with the most complex heart, blood vessel, and valve conditions. We have one of the highest success rates for cardiac catheterization procedures. Learn more about Cardiac Catheterization.

Help Kids and Make a Difference
Invest in future cures for some of life's most devastating diseases. Give today to help more children grow up stronger.

